
Trends in Assisted Peritoneal Dialysis in France Over 45 Years: Data from the RDPLF Registry
DOI:
https://doi.org/10.25796/bdd.v9i1.87103Keywords:
peritoneal dialysis, assisted peritoneal dialysis, CAPD, APD, home care nurseAbstract
Background
Assisted peritoneal dialysis (PD) has played an important role in France by enabling elderly and frail patients to access home dialysis despite limited autonomy, supported by the widespread involvement of home nursing care. The aim of this study is to describe the evolution of assisted PD in France using data from the RDPLF registry.
Methods
Incident PD patients recorded between 1981 and 2025 were analyzed and grouped into consecutive 5-year periods. For each period, we assessed the number of incident patients, the proportion receiving assisted treatment, and mean age, separately for continuous ambulatory PD (CAPD) and automated PD (APD).
Results
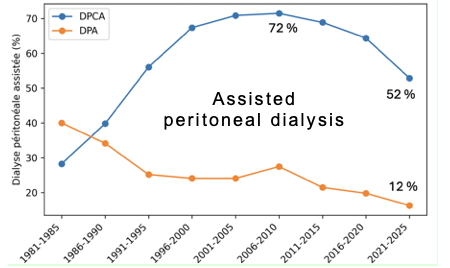
A total of 42,000 patients were included. The proportion of assisted CAPD patients increased steadily, peaking at around 72% between 2006 and 2010, before declining to 52% in recent years. In contrast, assisted APD decreased continuously, from approximately 40% in the early 1980s to 12% in 2025.
Discussioon: These trends were not related to patient age but were largely explained by a marked reduction in private nurse assistance. APD, more often used by younger patients, was consistently associated with greater autonomy. Over the last five years, PD incidence declined while the proportion of autonomous patients increased. The decrease in the incidence of PD in France could be linked to a preferential selection of independent patients, due to the reduced availability of private home nurses.
Conclusions
The evolution of assisted PD in France raises important public health concerns. Reduced access to home nursing care may limit access to PD for frail patients and hinder its development. The future of home dialysis depends on striking the right balance between patient autonomy and ongoing professional support.
Introduction
In 1974, the first patients treated with machine-assisted peritoneal dialysis were able to undergo dialysis at home because of the machine developed by Alain Slingeneyer in Professor Charles Mion’s department in Montpellier 1. A few years later, Popovich and Moncrief in Austin, Texas, advanced home peritoneal dialysis by developing a form of peritoneal dialysis known as equilibrium dialysis, which uses prolonged contact times of the dialysate in the peritoneal cavity, known as continuous ambulatory peritoneal dialysis (CAPD) 2. Many patients were negatively selected, that is, they were considered contraindicated for hemodialysis. Their weakness, therefore, generally required them to be assisted by their families. This constraint was not always well tolerated by couples; for this reason, in the early 1980s, private home nurses were paid by the social insurance fund to assist non-autonomous patients at home. A recent article by Rostoker et al. 3 sounded the alarm about the risks of a project that could eliminate the remuneration of private nurses for providing home care to peritoneal dialysis patients. In this context, we thought it would be interesting to look at the French home peritoneal dialysis and hemodialysis registry (RDPLF) to see how the care of peritoneal dialysis patients has evolved over the last 45 years.
Methods
Data source
This study is based on an analysis of data from the RDPLF. The database is hosted and managed using 4D SAS Quatrième Dimension software, version 20.7.
Study population
All adult incident patients (aged 18 or over) who started home peritoneal dialysis treatment in mainland France between January 1, 1981, and December 31, 2025, were included. A total of 42,163 incident patients were identified in the database.
Thirty-six records were excluded due to missing or clearly erroneous treatment start dates. The final population that was analyzed comprised 42,127 patients.
Variables and definitions
The following information was extracted for each patient:
· date of treatment initiation (incident patient)
· need for assistance in carrying out treatment
·type of assistance, classified into four categories
– no assistance (independent patient)
– assistance from a family member
– assistance from a nurse
– unspecified assistance
Patients were grouped into successive five-year periods between January 1, 1981, and December 31, 2025. For each five-year period, the following were calculated:
· the total number of incident patients
· the number of patients requiring assistance, by type of assistance
· the percentage in each category
Statistical analysis
Statistical analyses were performed using RStudio software with the R language (version 4.5.1). The results are presented in the form of descriptive tables and graphs. Graphical visualizations were produced using the ggplot2 package.
Results
Our analysis indicated changes in the percentage of assisted patients. Assistance was mainly extended to patients treated with DPCA, peaking between 2000 and 2010, then gradually declining while remaining proportionally higher than for those treated with DPA. The use of assistance in APD was higher than in CAPD, in percentage terms, in the 1980s only (Figure 1).
Figure 1.Change in the percentage of patients receiving home care with DPA and DPCA
The age of patients increased gradually over the first 10 yea rs, stabilizing at around 70 years from 1996 onwards, remaining nearly 20 years higher than the age of patients treated with APD. For the latter, the average age increased steadily from one period to the next Table I).
| Periods | All patients | CAPD | APD | |||
|---|---|---|---|---|---|---|
| No. of incidents | Average age (years) | No. of incidents | Average age (years) | No. of incidents | Average age (years) | |
| 1981–1985 | 667 | 57.6 ± 15.3 | 657 | 57.8 ± 15.2 | 10 | 48.5 ± 16.7 |
| 1986–1990 | 1,820 | 59.5 ± 17.1 | 1,747 | 59.8 ± 17.0 | 73 | 52.4 ± 16.7 |
| 1991–1995 | 3,851 | 64.1 ± 16.5 | 3,395 | 65.5 ± 15.9 | 456 | 53.8 ± 17.4 |
| 1996–2000 | 5,279 | 66.5 ± 16.4 | 4,092 | 70.1 ± 14.3 | 1187 | 54.2 ± 17.2 |
| 2001–2005 | 5,562 | 66.7 ± 17.1 | 3,689 | 72.1 ± 14.0 | 1873 | 56.1 ± 17.6 |
| 2006–2010 | 5,515 | 66.2 ± 17.5 | 3,197 | 72.8 ± 14.5 | 2318 | 57.2 ± 17.4 |
| 2011–2015 | 6,208 | 66.1 ± 17.6 | 3,706 | 72.7 ± 15.0 | 2502 | 56.7 ± 16.7 |
| 2016–2025 | 6,797 | 67.0 ± 16.7 | 4,406 | 72.1 ± 14.5 | 2391 | 58.0 ± 16.4 |
| 2021–2025 | 5,918 | 66.3 ± 16.2 | 3,757 | 70.4 ± 14.7 | 2161 | 59.1 ± 16.2 |
Care is mainly provided by private nurses, with family involvement remaining marginal. Nevertheless, whether in CAPD or APD, the percentage of independent patients is increasing in care, particularly in the last period (Figures 2 and 3). During this last period, the incidence of patients decreased in both CAPD and APD.
Figure 2.Evolution of autonomy in CAPD
Figure 3.Evolution of autonomy in APD
Discussion
Very early on, medical and nursing teams were made aware of the impact of dialysis on the spouse of the dialysis patient 4; these psychological aspects were more recently highlighted in the Bulletin de la Dialyse à Domicile 5. For this reason, mainland France was one of the first countries to develop assisted peritoneal dialysis, mainly thanks to a large network of private nurses whose home visits were covered by health insurance 6. The significant difference in the level of autonomy between patients treated with CAPD and APD can be explained by the age difference of almost 10 years. Patients treated with APD are often those who maintain an active social and professional life and for whom nocturnal dialysis on a machine frees up their entire day. Currently, more than 50% of patients treated with CAPD in France receive assistance from private nurses, with the level of assistance in APD being less than 20%, which allows patients who would otherwise undergo hemodialysis in a center to remain at home. Boyer et al. 7 showed that the incidence of nurse-assisted peritoneal dialysis increased following financial incentives in 2011 for this type of care; however, their study was an annual follow-up and ended in 2015. This probably explains why the present study does not confirm the long-term trend they demonstrated because our findings show that the increase in incidence reverses from 2015 in CAPD and from 2020 in APD. The influence of changes in the strategies of reimbursement by certain health insurances, as suggested in Rostoker’s recent article [3], should be evaluated. The last five years have been marked by a decrease in incidence regardless of the method and, in both cases, associated with a decrease in the percentage of patients assisted by nurses regardless of the technique. As it stands, this study has several limitations: The data are essentially descriptive, and a more in-depth analysis would be useful to confirm the observed trend; nevertheless, the overall decline in the incidence of PD has recently been confirmed at the European level 8. We limited the study to metropolitan France, and the role of the family may be very different in other regions or countries. The causes are probably not clear-cut: The availability of private nurses may be lower and should be studied, and spouses may have more comorbidities associated with increased frailty, reducing their ability to act as caregivers; thus, teams may prefer to select autonomous patients. The revival of APD is based on a paradigm shift, with a preference for identifying patients who are less autonomous or non-autonomous to whom the technique would be offered, combined with new measures to facilitate the use of private nurses.
Conclusion
The evolution of home care arrangements for patients treated with peritoneal dialysis in France has changed significantly over the last 45 years. Until the end of 2010, private nurses played a key role in providing home treatment for non-independent patients. However, since 2010, the percentage of patients assisted by private nurses has been decreasing gradually, which is associated with a decrease in the incidence of peritoneal dialysis prescriptions. Keeping non-autonomous patients at home will require an adaptation of health policy to promote the care of these patients.
GENERAL STATEMENTS
Authors’ Contributions
CV exported the data, performed the statistical analysis, and wrote the article; JC proofread the article, provided constructive comments, and made corrections; EF created the database, maintained it, proofread the article, and provided comments.
Ethical Considerations and patient consent
This is a retrospective study based on a registry declared to the French Data Protection Authority (CNIL) under number 542668.
It was a cross-sectional observational study conducted without any medical or therapeutic intervention, using anonymized data.
Data availability
The original data used in this study are available from the RDPLF secretariat within the limits of a reasonable request.
Funding
The authors did not receive any funding for this work.
Conflicts of Interest
The authors declare no conflict of interest with this work
Acknowledgments
We thank the French-speaking nursing and medical teams for their trust and the consistent quality of their updates over the past 45 years.
We thank Ms. Katia Guerin for formatting the BDD articles and for her secretarial work.
We thank Ms. Ghislaine Veniez, nurse, for her ongoing quality control of the data.
ORCID iDs
Christian Verger: https://orcid.org/0000-0002-8009-5366
Jacques Chanliau: https://orcid.org/0009-0008-8454-8271
Emmanuel Fabre : https://orcid.org/0000-0003-4256-0500
Copyright & License
© 2026 Christan Verger, Chanliau Chanliau, Emmanuel Fabre.
This work is licensed under a Creative Commons Attribution 4.0 International License.

References
1. Verger C, Chanliau J. History of peritoneal dialysis in France. Bull Dial Domic [Internet]. 2019 Sep. 13 [cited 2026 Jan. 10];2(3):119-25. Available from doi: https://doi.org/10.25796/bdd.v2i3.22103 DOI: https://doi.org/10.25796/bdd.v2i3.22103
2. Popovich RP, Moncrief JW, Nolph KD, Ghods AJ, Twardowski ZJ, Pyle WK. Continuous ambulatory peritoneal dialysis. Ann Intern Med. 1978 Apr;88(4):449-56. doi: https://doi.org/10.7326/0003-4819-88-4-449 DOI: https://doi.org/10.7326/0003-4819-88-4-449
3. Rostoker G, Issad B, Pittion-Marin J, Fessi H. Assisted peritoneal dialysis in France threatened by restrictive interpretation of legislation by CPAM?. Bull Dial Domic [Internet]. 2025 Dec. 17 [cited 2026 Jan. 10];8(4):295-8. Available from doi: https://doi.org/10.25796/bdd.v8i4.87089 DOI: https://doi.org/10.25796/bdd.v8i4.87089
4. Streltzer J, Finkelstein F, Feigenbaum H, Kitsen J, Cohn GL. The spouse’s role in home hemodialysis. Arch Gen Psychiatry. 1976 Jan;33(1):55-8. doi: https://doi.org/10.1001/archpsyc.1976.01770010033006. DOI: https://doi.org/10.1001/archpsyc.1976.01770010033006
5. Roques M, Proia-Lelouey N. La dialyse à domicile : une dynamique interactive complexe pour les couples. Bull Dial Domic [Internet]. 23 sept. 2018 [cité 19 janv. 2026];1(2):83-7. available at doi: https://doi.org/10.25796/bdd.v1i2.51 DOI: https://doi.org/10.25796/bdd.v1i2.51
6. Durand PY, Verger C. The state of peritoneal dialysis in France. Perit Dial Int. 2006 Nov-Dec;26(6):654-7. PMID: 17047231. DOI: https://doi.org/10.1177/089686080602600608
7. Boyer A, Lanot A, Lambie M, Guillouet S, Lobbedez T, Béchade C. Trends in assisted peritoneal dialysis over the last decade: a cohort study from the French Peritoneal Dialysis Registry. Clin Kidney J. 2020 May 17;13(6):1003-1011. doi: https://doi.org/10.1093/ckj/sfaa051 DOI: https://doi.org/10.1093/ckj/sfaa051
8. Slon-Roblero MF, Stel VS, Sanchez-Alvarez E, Escola JM, Dias BJF, Auñón AS, Ferraro PM, De Meester JM, Boyer A, Rydell H, Hommel K, Åsberg A, Arias IR, Methven S, Huete MJE, Abrahams AC, Palsson R, Goffin E, Aresté-Fosalba N, Bello AJ, Kuzema V, Helve J, Kerschbaum J, Bakkaloglu SA, Kislikova M, Jager KJ, Ortiz A, Kramer A. Trends in Home Dialysis Over the Last Decade in Europe: an ERA Registry Study. Nephrol Dial Transplant. 2025 Aug 29:gfaf171. doi: https://doi.org/10.1093/ndt/gfaf171 DOI: https://doi.org/10.1093/ndt/gfaf171
Downloads
Submitted
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 Christan Verger, Chanliau Chanliau, Emmanuel Fabre

This work is licensed under a Creative Commons Attribution 4.0 International License.



